 EN
EN  DE
DE  ES
ES  FR
FR 
Postural balance
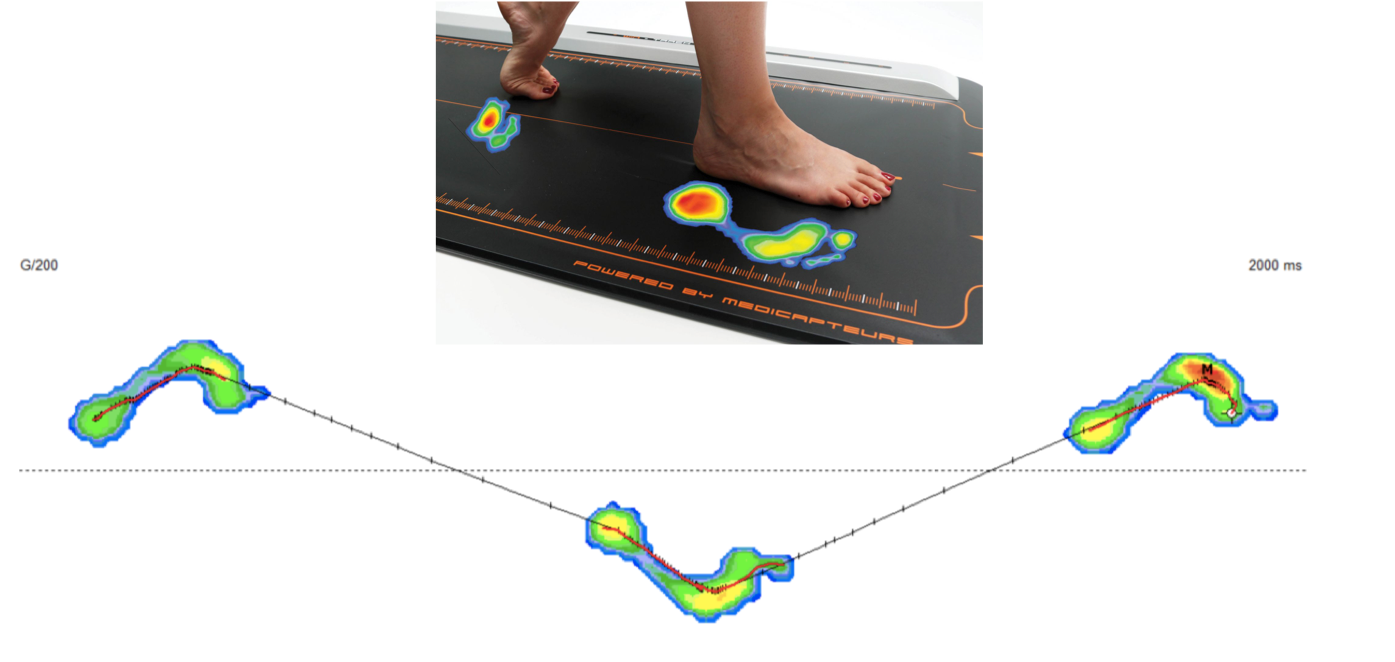
FHL induces a postural imbalance that can be clinically seen by placing the patient in unipodal support. This imbalance results in a displacement of the projection of the center of gravity towards the rear and towards the outside of the foot that we can see on a loading or walking platform, is what has been carried out on hundreds of patients as part of our check-ups before and after surgery (tenolysis of the flexor digitorum longus).
Dynamic balance and synchronism when walking
During the walking cycle, the foot and ankle will perform alternating tilting movements of supination over pronation and pronation over supination at specific times of the cycle. Pronation is characterized by an inward tilt of the foot and, conversely, supination is an outward movement of the foot. Switching from one position to another is usually a smooth process.
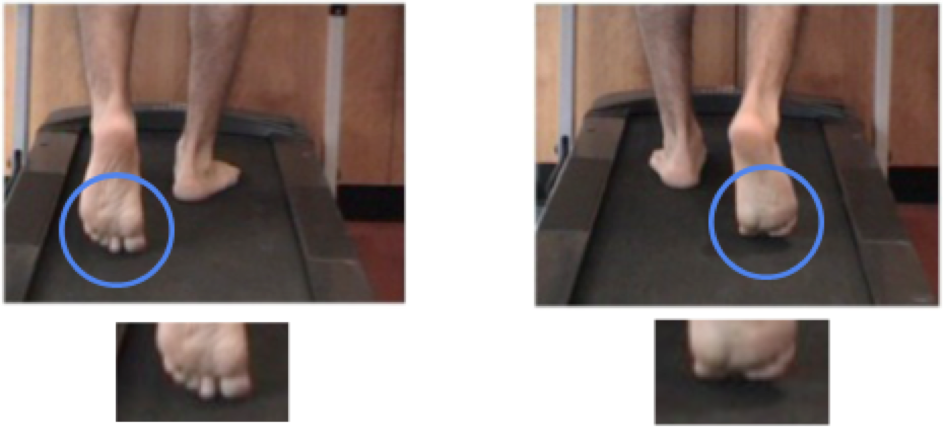
Our analysis has shown that this tilt observed at the end of the support phase is much more abrupt (true break) in the presence of FHL. The resulting functional disturbances result in over-stressing of all the joints of the lower limb up to the lumbar spine, explaining both the so-called overload lesions which also promote acute accidents. One serious and common injury associated with this phenomenon is the tearing of the anterior cruciate ligament.
In this chapter devoted to the local and remote repercussions of FHL, we must consider that the action of walking is a synchronous movement which positions the body in a given attitude during putting weight on the foot, alternately left and right. The body passes over the foot in a motion that is analogous to that of an inverted pendulum. Each moment of the passage corresponds to a weight under the foot which moves from back to front until the propulsion. In case of exaggerated or time-delayed pronation or supination, the position of the body must adapt and try to compensate for the imbalance.
This is not always possible, especially for the knee, because its anatomy does not allow it to correct a rotational disorder. The muscles are put to a greater contribution, in particular the bi-articular muscles. But here again, the situation is made delicate by a body posture which makes the contraction less efficient and often shifts the start of the contraction. In summary, this is a complex phenomenon that still needs to be correlated with the age, bone architecture and the muscular and morphological condition of each individual to assess the impact on functioning in order to understand the clinical implications. The analysis of gait and the podiatry assessment on the treadmill are our most valuable diagnostic tools.
Learn more
 Approche thérapeutique globale et apports de la podologie
Approche thérapeutique globale et apports de la podologie  Intérêt du bilan de marche et du bilan fonctionnel
Intérêt du bilan de marche et du bilan fonctionnel  The child’s foot
The child’s foot Intérêt de l'analyse instrumentalisée de la marche
Intérêt de l'analyse instrumentalisée de la marche  Research: FHL and Gait Analysis
Research: FHL and Gait Analysis